


WHY SPINRAZA/LATER-ONSET STUDIES

Considering treatment?
SPINRAZA has been studied for over a
decade in the longest SMA clinical development program to date


People with later-onset SMA treated with SPINRAZA showed significant improvements in motor function in the CHERISH study
In clinical studies, on average, individuals with later-onset SMA treated with SPINRAZA experienced maintenance of, or even saw improvements in, current muscle function.
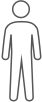
People on SPINRAZA had a 3.9-point improvement in overall motor function versus a 1.0-point decline in the untreated control group.
Pivotal study: CHERISH
Who: 126 individuals aged 2 to 9 years with later-onset SMA
Study time: 15 months
Primary outcome: Changes in motor function measured on the HFMSE
Secondary outcome: Changes in upper limb function measured on the RULM and percentage of individuals who had a clinically meaningful improvement of 3 or more points from baseline in HFMSE score
Limitation: The dosing schedule was different than the approved SPINRAZA schedule
Safety: The most common side effects were fever (43%), headache (29%), vomiting (29%), and back pain (25%)
The pivotal trial that proved SPINRAZA significantly improves function in children with later-onset SMA versus untreated control group
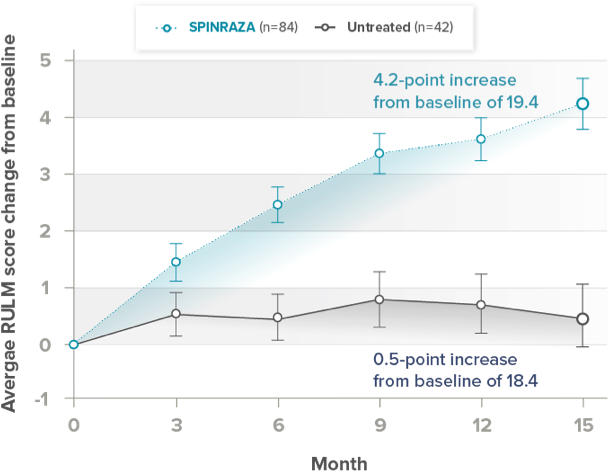
Primary outcome: Average change from baseline in HFMSE total score at 15 months versus untreated individuals
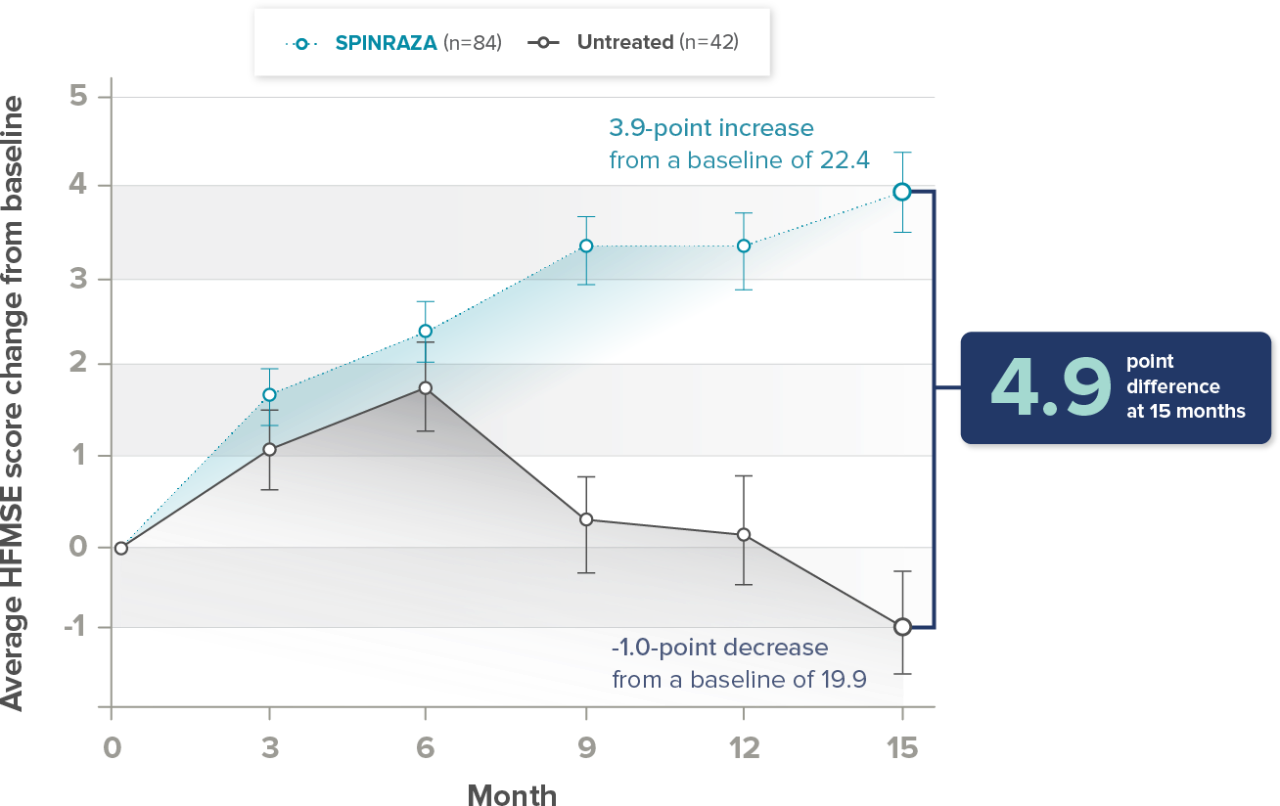
A 1- or 2-point improvement on HFMSE is considered a positive change, and ≥3-point improvement a clinically meaningful change
Average results in the SPINRAZA group showed significant improvement in their motor function. Motor function began to steadily improve in just 9 months as compared to the untreated group.
Secondary outcome: Percentage of individuals with a ≥3-point increase from baseline in HFMSE score
56.8% of the 84 individuals treated with SPINRAZA
26.3% of the 42 in the untreated control group
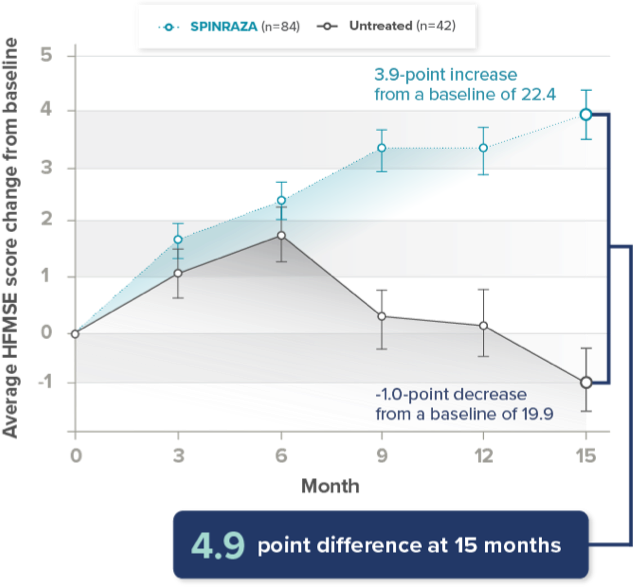
Secondary outcome: Average change from baseline in upper limb function score at 15 months
A real-world study for older children and adults on SPINRAZA with an extensive follow-up period of up to 30 months
Łusakowska Study
This study was supported by a grant from Biogen.
This study looked at how well patients were doing in different activities, using different assessments dependent on their functional abilities (HFMSE [n=73 ambulatory and sitters], RULM [n=51, used for nonambulatory and ambulatory patients], CHOP INTEND [n=47, used for non or weak sitters], 6MWT [n=27], and PGI-I [n=120]).
Highlights of the study:
- Included 120 children and adults (5 to 66 years old) with SMA (Types 1c-3)
- One of the longest real-world studies, with individuals assessed for up to 30 months
- Most individuals (74%) had SMA Type 3, and the average age at baseline was 32 years
- Safety reported in the study is generally consistent with the safety reported in the SPINRAZA clinical trials
Limitations of the study: Observational study that does not include a comparison with an untreated group. This type of study is valuable, but not as strong as a pivotal study.
The study was conducted at multiple treatment centers in Poland; practices may vary by country.
Only 12 participants had SMA Type 1c and 19 had SMA Type 2.
The dosing schedule in the study was different from the approved SPINRAZA schedule.
Missing data for some timepoints, some due to COVID, some because patients had not yet reached those timepoints.
The scale used to measure self-reported improvement (PGI-I) relies on what patients say and hasn’t been proven in SMA.
Average results showed improvement in motor function at each timepoint compared with baseline


HFMSE patient population (n=73):
Average age:
31 years
SMA Type 2:
6 patients
(4 children)
SMA Type 3:
67 patients
(10 children)
- Over the course of treatment, average HFMSE scores showed improvements compared with baseline, ranging from 2.5 points at 6 months (n=72) to 5.1 points (n=28) at 30 months
- Proportion of patients experiencing no change from baseline ranged from 8% to 20% during the study
- Proportion of patients experiencing worsening from baseline ranged from 1.5% to 8% during the study
Average results showed improvements in walking ability based on the 6MWT at each timepoint


6MWT patient population (n=27):
Average age:
27 years
SMA Type 3:
27 patients
- Results were variable, but over the course of the study, average 6MWT scores showed improvements compared with baseline, ranging from 5.4 meters, or 17.7 feet (n=15), at 6 months to 27 meters, or 88.5 feet (n=12), at 30 months
- Proportion of patients experiencing no change from baseline ranged from 0% to 7% during the study
- Proportion of patients experiencing worsening from baseline ranged from 14% to 50% during the study
Patients and caregivers assessed and self-reported their status utilizing the PGI-I
At various points during the study:
75% to 88%
of patients reported an improvement
9% to 24%
of patients reported no change
0% to 5%
of patients reported feeling minimally worse
No patients
reported feeling much worse or very much worse
Safety reported in the study was generally consistent with the safety reported in the SPINRAZA clinical trials. Common side effects include lower respiratory infection, fever, constipation, headache, vomiting, back pain, and post-lumbar puncture syndrome.
A real-world study for teens and adults on SPINRAZA with a follow-up period of up to 38 months
SMArtCARE Study
This study assessed 3 functional outcome measures: HFMSE (clinically meaningful improvement defined as a change of ≥3 points), RULM (clinically meaningful improvement defined as a change of ≥2 points), and 6MWT (for ambulatory individuals, clinically meaningful improvement defined as an increase in walking distance by ≥30 meters).
Highlights of the study:
- Included 237 teens and adults between the ages of 16 and 71 years old, with an average age of 36 years*
- One of the longest real-world evidence studies, with individuals assessed for up to 38 months
- Included individuals with SMA Types 1, 2, 3, and 4
*Functional outcomes were assessed at baseline, 14, 26, and 38 months of treatment.
Limitations of the study: Observational study does not include a comparison with an untreated group. This type of study is valuable, but not as strong as a pivotal study.
Limited to patients from 3 countries–Austria, Germany, Switzerland; practices may vary by country.
Limitations of HFMSE and RULM in capturing the full range of possible responses.
The dosing schedule in the study was different from the approved SPINRAZA schedule.
*Functional outcomes were assessed at baseline, 14, 26, and 38 months of treatment.
Average results showed improvement in motor function at each timepoint compared with baseline*
Primary endpoint: Change in HFMSE from baseline
Average Improvement:
1.72
14 MONTHS
(N=237)
1.20
26 MONTHS
(N=171)
1.52
38 MONTHS
(N=120)
*At baseline, 2 patients had a full score (66 points) and 55 patients scored 0 points.
Proportion of patients with clinically meaningful change in HFMSE score vs baseline up to 38 months


- Clinically meaningful improvement is ≥3 points
- Clinically meaningful worsening is –3 points or more
- 41% of patients (28/68) with clinically meaningful improvement in HFMSE score at 14 months maintained this improvement for ≥38 months†
- Clinically meaningful worsening n HFMSE score was seen in 8%, 15%, and 13% of patients at 14, 26, and 38 months, respectively
†Functional outcomes were assessed at baseline, 14, 26, 38 months of treatment.
Average results showed improvements in upper limb function at each timepoint compared with baseline*
Average improvement in RULM from baseline
Average Improvement:
0.75
14 MONTHS
(N=237)
0.65
26 MONTHS
(N=173)
0.72
38 MONTHS
(N=123)
*At baseline, 74 patients had a full score (37 points) and 17 patients scored 0 points.
Proportion of patients with clinically meaningful change in RULM score vs baseline up to 38 months


- Clinically meaningful improvement (≥2 point increase)
- Clinically meaningful worsening (–2 points or more)
- 37% of patients (25/68) with clinically meaningful improvement in RULM score at 14 months maintained this improvement at 38 months†
- Clinically meaningful worsening in RULM score was seen in 11%, 13% and 7% of patients at 14, 26, and 38 months, respectively
†Functional outcomes were assessed at baseline, 14, 26, 38 months of treatment.
Regardless of ambulatory status, improvement in average HFMSE and RULM scores were reported with SPINRAZA.
Safety reported in the study is generally consistent with the safety reported in the SPINRAZA clinical trials. Common side effects include lower respiratory infection, fever, constipation, headache, vomiting, back pain, and post-lumbar puncture syndrome.
Supportive studies: CS2/CS12
Who: 28 individuals aged 2 to 15 years with later-onset SMA treated with SPINRAZA
Study time: approximately 3 years
Primary outcome: These supportive studies were designed to determine the safety of SPINRAZA
Other outcomes: The safety and longer-term effects of SPINRAZA on overall motor function, upper limb function and walking ability were also studied
Limitations: The dosing was different than the approved SPINRAZA schedule. Additionally, these studies had no untreated control group and a small number of participants and so may not be as reliable as the clinical trial data.
This type of study is valuable, but not as strong as a pivotal study.
Safety: Side effects were consistent with those reported in the pivotal trials
The longer-term effect of SPINRAZA on overall motor function, upper limb function, and walking ability was measured over 3 years
Average changes in motor function*
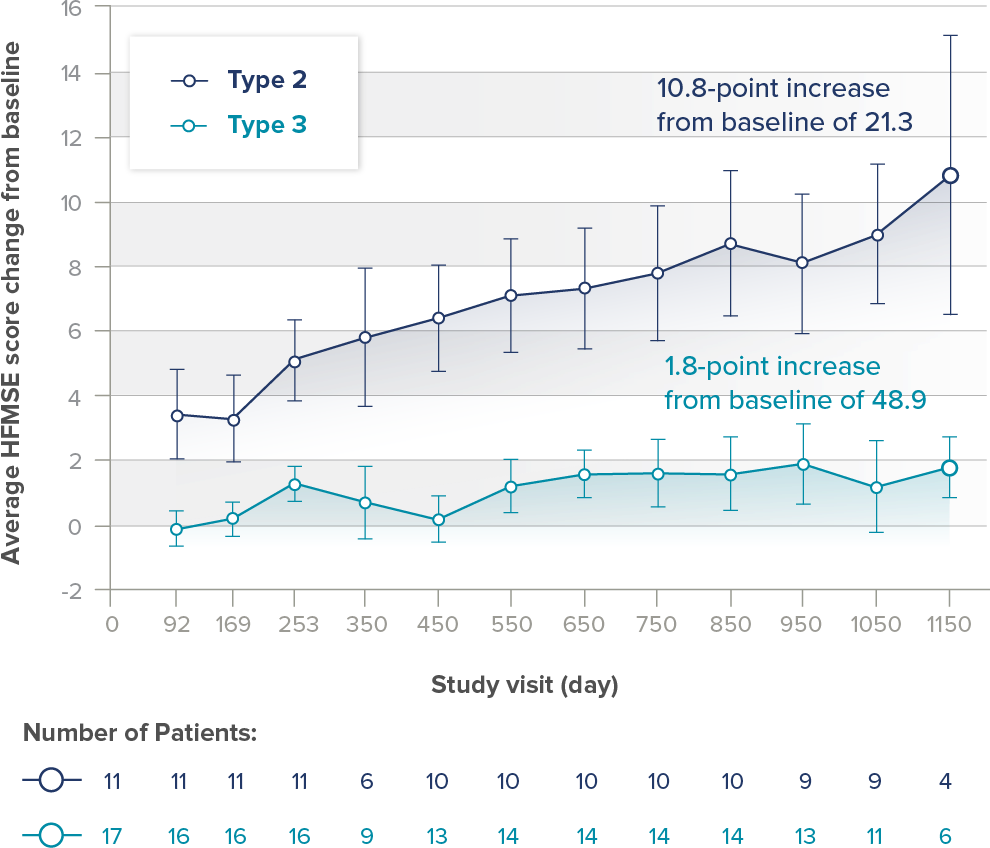
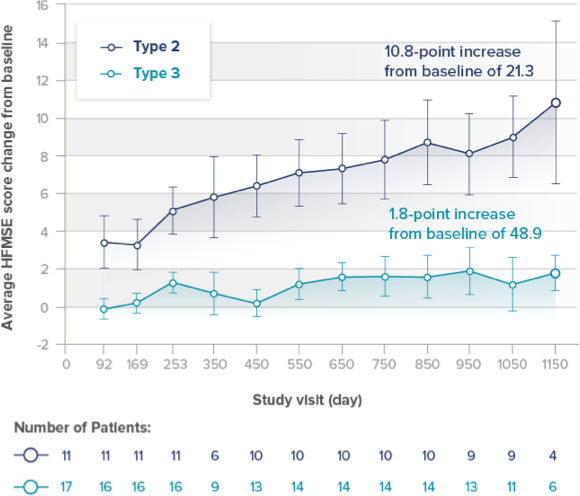
*Due to a gap between study visits, some data points do not contain results for all children.
Average changes in upper limb function in nonambulatory individuals treated with SPINRAZA


56% (5/9) individuals saw clinically meaningful improvements in ULM by approximately year 3 (Defined as ≥2-point increase from baseline†)
†Due to a gap between study visits, some data points do not contain results for all children.
100% (8/8) of people who had the ability to walk achieved improvements in their walking distance by approximately year 3 (improvements defined as ≥30 meters from baseline)‡
‡Due to a gap between study visits, some data points do not contain results for all children.


1 of the 11 with Type 2 SMA gained the ability to walk.
2 of the 4 with Type 3 SMA regained the ability to walk.
§day 1150 n=5


“Having SMA, I set the example by doing things that could be perceived as difficult. Yeah, I still have SMA, but I don't let SMA stop me.”